
Dental Implants vs Dentures vs Bridges: An Honest Side-by-Side

Dental Implants vs Dentures vs Bridges: An Honest Side-by-Side
When a Tooth Is Lost, the Real Decision Begins
Losing a tooth — whether to decay, fracture, gum disease, or planned extraction — is the beginning of a decision process that many patients feel underprepared for. The dentist mentions implants, bridges, and dentures, and the patient leaves with a vague sense that implants are the expensive option, bridges are the middle ground, and dentures are for older people. Beyond that, the picture is often unclear.
That lack of clarity leads to decisions based on the wrong criteria — usually upfront cost — without fully accounting for what each option involves, how long it lasts, what it does (or does not do) for the bone beneath the gum, and how it will feel to live with it over a decade or more.
This guide gives you an equal and honest account of all three options. There is no single right answer that applies to every patient — each option has genuine advantages and genuine limitations, and the best choice depends on clinical factors, lifestyle, and what the patient values most. What this guide can do is make sure you are asking the right questions and understand the full picture before committing to any one path.
🔑 Key Takeaways
- All three options — implants, bridges, and dentures — can effectively replace missing teeth, but they differ fundamentally in how they interact with the jawbone, adjacent teeth, and daily function.
- Implants are the only option that preserves jawbone by replacing the tooth root. Both bridges and dentures allow bone resorption to continue beneath the gap.
- A bridge requires the permanent alteration of two healthy adjacent teeth, which become crowned for life. This is a significant and irreversible commitment that patients do not always fully appreciate before proceeding.
- Dentures carry the lowest upfront cost but require the most ongoing management — adjustments as the bone ridge changes, cleaning routines, removal at night, and eventual replacement as fit changes.
- The long-term cost of each option — accounting for replacement, maintenance, and the management of consequences — is often closer than the upfront figures suggest.
- The decision is always made in the context of the whole mouth: how many teeth are missing, what the bone levels are, the condition of adjacent teeth, and the patient’s overall oral health goals.
Option 1: Dental Implants
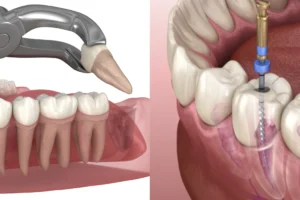
A dental implant is a titanium fixture — typically shaped like a small screw — that is surgically placed into the jawbone to replace the root of the missing tooth. Once the implant has integrated with the bone through a process called osseointegration (typically over three to six months), a ceramic crown is attached to the top of the implant. The result is a tooth replacement that looks, feels, and functions like a natural tooth — and is anchored in the jaw in the same way a natural tooth root is.
How the Procedure Works
Implant placement is a surgical procedure carried out under local anaesthesia and, where appropriate, sedation. The implant fixture is placed into the prepared bone site, the gum is closed over it, and a healing period follows — during which the bone grows around and bonds to the titanium surface. At Nova Dental Hospital, a pre-implant assessment using a CBCT 3D scan evaluates the bone volume, bone quality, and proximity to anatomical structures before placement is planned. This imaging step is important for surgical accuracy and for identifying in advance whether bone grafting is needed.
After osseointegration is confirmed, an abutment is attached to the implant fixture, and the final crown is fitted. The crown is colour-matched to the adjacent teeth and is fixed — not removable. The total treatment time from implant placement to final crown is typically four to eight months for a straightforward single-tooth case.
The Key Advantage: Bone Preservation
The defining biological advantage of an implant over every other replacement option is bone preservation. The jawbone maintains its density and volume through the stimulation provided by tooth roots under biting load. When a root is removed and nothing replaces it, the bone in that area begins to resorb — to shrink. An implant provides the same stimulation that a natural root did, preventing this resorption and maintaining the bone volume and facial contour in the area. Neither a bridge nor a denture can do this, because neither replaces the root.
Who Dental Implants Are Best Suited For
- Patients who are missing one or more teeth and want the closest functional and aesthetic equivalent to natural teeth.
- Patients with adequate bone volume in the jaw — or who are willing to undergo bone grafting if volume is insufficient.
- Patients who are non-smokers, or willing to stop smoking around the procedure — smoking significantly impairs osseointegration.
- Patients with well-controlled general health — certain conditions such as uncontrolled diabetes affect healing and implant success rates.
- Patients taking a long-term view — implants have the highest upfront cost of the three options but the best longevity and the lowest long-term maintenance burden when successful.
Limitations and Considerations
- Surgical procedure required: Implant placement is surgery. It carries the standard surgical considerations around healing, infection risk, and the rare possibility of complications.
- Healing time: The osseointegration period means the treatment timeline is measured in months rather than weeks. Patients who need a replacement quickly may require a provisional solution in the interim.
- Bone volume: Insufficient bone — particularly in patients who had a tooth extracted some time ago and have experienced resorption — may require bone grafting before implant placement, adding cost and time.
- Not suitable for all patients: Patients with certain medical conditions, those on specific medications (notably bisphosphonates), and heavy smokers require individual clinical assessment before implants are recommended.
Option 2: Dental Bridge
A dental bridge is a fixed prosthetic that replaces one or more missing teeth by spanning the gap and anchoring to the natural teeth on either side of it. The adjacent teeth — called abutment teeth — are permanently reduced in size and crowned. An artificial tooth (or teeth), called a pontic, is suspended between the two crowns, filling the gap. The bridge is cemented in place and is not removable.
The bridge is a well-established and effective tooth replacement. It restores appearance and function, does not require surgery, and can be completed in a shorter timeframe than an implant — typically two to three appointments over two to three weeks.
How the Procedure Works
The abutment teeth are prepared — reshaped by removing a layer of enamel and dentine from all surfaces — to create the foundation for the bridge crowns. An impression or digital scan is taken and sent to the laboratory for fabrication of the bridge. A temporary bridge is placed while the permanent one is made. At the fit appointment, the bridge is cemented and adjusted for bite.
The Critical Consideration: Commitment of Adjacent Teeth
The most significant clinical consideration with a bridge is what it does to the adjacent healthy teeth. To serve as bridge abutments, these teeth must be permanently prepared — ground down on all surfaces to receive the bridge crowns. Once this is done, those teeth require crowning for the rest of the patient’s life. If the bridge ever needs to be replaced, the abutment teeth are already prepared and will need new crowns. If the abutment teeth develop problems — decay under the crown, nerve damage from the preparation, gum recession — the entire bridge is compromised.
For a patient whose adjacent teeth are already crowned or heavily restored, a bridge may represent a practical and straightforward option — the existing crowns are being replaced or extended in function. For a patient with healthy, unrestored adjacent teeth, the bridge requires sacrificing the intact structure of two teeth to replace one missing one — a significant irreversible commitment that is worth weighing carefully.
Bone Resorption Beneath a Bridge
A bridge replaces the visible tooth but not the root. The bone beneath the pontic — the artificial tooth suspended in the gap — continues to resorb over time because there is no root stimulating it. This resorption eventually creates a visible gap between the gum and the underside of the pontic, changing the appearance of the bridge. It also affects the contour of the face in the area over the long term, particularly in the front of the mouth.
Who a Dental Bridge Is Best Suited For
- Patients who are not surgical candidates for implants due to medical conditions or insufficient bone that cannot be grafted.
- Patients whose adjacent teeth are already crowned or significantly restored — the preparation commitment is reduced when those teeth already need crowning.
- Patients who prefer a shorter treatment timeline and want a fixed (non-removable) result without surgery.
- Patients replacing one or two missing teeth in a position where the adjacent teeth are strong enough to carry the additional load.
Limitations and Considerations
- Permanent alteration of adjacent teeth: The most significant limitation — healthy adjacent teeth are permanently prepared, committing them to crowns for life.
- No bone preservation: Bone continues to resorb beneath the pontic, affecting the fit and appearance of the bridge over time.
- Cleaning challenges: Flossing under a bridge requires a floss threader or interdental brush — patients who do not clean beneath the bridge are at risk of decay and gum disease at the margins.
- Longevity: A well-maintained bridge typically lasts 10 to 15 years before requiring replacement. When it is replaced, the abutment teeth are prepared again.
Option 3: Dentures
A denture is a removable prosthetic — a plate, typically made of acrylic, that carries artificial teeth and sits on the gum ridge. A partial denture replaces one or several missing teeth among remaining natural teeth. A complete denture replaces an entire arch when all teeth are missing. Both types rest on the gum tissue and, where applicable, are retained by clasps on remaining natural teeth or by suction and adhesive.
Dentures have the lowest upfront cost of the three options and can be made relatively quickly — often within a few weeks of impressions being taken. They are the most accessible option for patients who cannot or do not wish to undergo surgery, and for patients who are missing many teeth across an arch.
How Dentures Work
Impressions of the gum ridges and remaining teeth are taken and used to fabricate the denture in a laboratory. Several appointments are typically needed to achieve a good fit and correct bite. The denture is removed at night for cleaning and to allow the gum tissue to rest. As the bone ridge beneath a denture changes shape over time — due to ongoing resorption — the fit of the denture changes and periodic relining or replacement is required.
Implant-Retained Dentures: The Middle Ground
An important variation is the implant-retained denture — sometimes called an overdenture — in which two or more implants are placed in the jaw and the denture clips onto them. The denture is still removable, but the implants provide secure retention that eliminates movement and dramatically improves biting force and confidence. The implants also help slow bone resorption in the areas where they are placed. For patients who need a full arch replacement and want more stability than a conventional denture provides without the cost of a fully fixed implant bridge, an implant-retained denture represents a practical and effective middle option. At Nova Dental Hospital, full mouth rehabilitation planning accounts for both fixed and removable implant-supported options.
Who Dentures Are Best Suited For
- Patients who are missing many teeth across one or both arches, where implants for each individual tooth would be clinically complex or cost-prohibitive.
- Patients who are not surgical candidates and for whom a bridge is not viable due to the position or number of missing teeth.
- Patients who need a temporary solution while planning a longer-term restoration.
- Elderly patients with limited bone volume and medical complexities where a removable solution is the most practical approach.
Limitations and Considerations
- Removable: Dentures must be removed at night and for cleaning. Some patients find this adjustment significant — particularly the first full denture.
- Movement during function: Conventional dentures — particularly lower full dentures — can move during eating and speaking without implant support. Adhesive is commonly used but does not fully replicate the stability of a fixed restoration.
- Bone resorption continues: Dentures do not address bone resorption beneath the gum. The ridge changes over time, altering the fit. This is most pronounced in the first year after tooth loss and continues, albeit more slowly, thereafter.
- Ongoing adjustment: As the ridge changes, the denture needs relining or remaking — typically every five to seven years for a well-maintained denture.
- Reduced biting force: Conventional dentures transmit force through the gum tissue rather than the bone, which significantly reduces effective biting force compared to natural teeth or implant-retained restorations.
The Complete Comparison: Implants, Bridges, and Dentures Side by Side
| Dental Implant | Dental Bridge | Denture | |
| Replaces the root | Yes — titanium root in the jaw | No | No |
| Preserves jawbone | Yes — implant stimulates bone | No — bone resorbs beneath pontic | No — bone resorbs beneath plate |
| Fixed or removable | Fixed (cemented crown) | Fixed (cemented bridge) | Removable |
| Effect on adjacent teeth | None — standalone restoration | Adjacent teeth permanently prepared and crowned | Partial denture clasps on adjacent teeth; full denture has no adjacent teeth |
| Procedure type | Surgical | Non-surgical | Non-surgical |
| Treatment timeline | 4–8 months (single tooth) | 2–3 weeks | 3–6 weeks |
| Biting force | Equivalent to natural tooth | Good — reduced slightly at pontic | Significantly reduced vs. natural teeth |
| Appearance | Indistinguishable from natural | Very natural; minor gum gap over time | Good initially; changes as ridge resorbs |
| Cleaning | Brush and floss as normal | Requires floss threader under bridge | Remove and clean separately; soak overnight |
| Longevity | 20+ years with good care; often lifetime | 10–15 years typically | 5–8 years before reline or replacement |
| Bone grafting sometimes needed | Yes — if insufficient bone | No | No |
| Upfront cost | Highest | Moderate | Lowest |
| Long-term total cost | Often lowest over 20+ years | Moderate (bridge replacement cycles) | Ongoing adjustment and replacement costs |
| Best for | Single or multiple missing teeth; patients prioritising longevity and bone health | 1–2 missing teeth with already-compromised adjacent teeth; non-surgical candidates | Multiple missing teeth; full arch replacement; non-surgical or budget-first patients |
Understanding the True Cost of Each Option
Cost is typically the first question patients ask, and upfront figures can be misleading if they are not placed in the context of longevity and ongoing maintenance. A fair cost comparison accounts for the full treatment pathway — not just the initial procedure.
Implants: High Upfront, Low Long-Term
Dental implants carry the highest initial cost of the three options. The cost encompasses the implant fixture, the abutment, the crown, and the pre-implant diagnostic workup — including, where indicated, a CBCT 3D scan for precise surgical planning. If bone grafting is required, this adds further to the initial cost.
However, a well-placed implant with a good-quality crown, maintained with regular dental care, can last twenty years or more — often a lifetime. It does not require the adjacent teeth to be prepared, does not need relining as the bone changes, and its maintenance cost over ten or twenty years is primarily the cost of regular check-ups and professional cleaning. When the total cost of ownership is modelled over, say, fifteen to twenty years, an implant is often the most cost-efficient option of the three.
Bridges: Moderate Cost, Replacement Cycles
A bridge is less expensive than an implant upfront and is completed faster. However, bridges have a finite lifespan — typically ten to fifteen years for a well-maintained bridge — after which they need to be replaced. Each replacement cycle involves new preparation of the abutment teeth (which are increasingly compromised with each cycle), new laboratory work, and a new cost. Over a twenty-year horizon, the combined cost of two bridge replacements can approach or exceed the one-time cost of an implant, without the bone preservation benefit.
Dentures: Lowest Upfront, Most Ongoing
Dentures are the least expensive option initially and are the fastest to provide. But they require the most ongoing management: periodic relining as the bone ridge changes, replacement when the fit degrades beyond relining, replacement teeth as they wear or break, and the associated appointments. For a patient who will wear a denture for twenty or thirty years, the cumulative cost of maintenance and replacement is significant — and the functional and aesthetic compromises of a conventional denture remain throughout.
Patients are always welcome to discuss the realistic cost picture for their specific situation in a general dentistry consultation at Nova Dental Hospital, where the clinical assessment, bone volume, and treatment options can be reviewed in full.
When Multiple Teeth Are Missing
The comparison above addresses single-tooth replacement, but the picture changes when multiple teeth are missing — particularly across an entire arch.
Implant-Supported Bridge (Full Arch)
When all or most teeth in an arch are missing, a full-arch implant-supported bridge — sometimes referred to by brand names such as All-on-4 or All-on-6 — provides a fixed, non-removable full arch of teeth supported by four to six strategically placed implants. This approach provides the stability and function of fixed teeth at a fraction of the cost of individual implants for every tooth. It is one of the most significant advances in restorative dentistry for patients who have lost most or all of their teeth, and it is assessed as part of full mouth rehabilitation planning.
Implant-Retained Overdenture
For patients who want improved stability over a conventional denture without the cost of a fully fixed implant solution, two to four implants can be placed to serve as anchors for a removable overdenture. The denture clips onto the implants, eliminating the movement that makes conventional dentures challenging during eating and speaking. This option retains the practicality of a removable prosthetic while delivering a step-change in comfort and confidence.
Multiple Bridges
Multiple adjacent missing teeth can be replaced with a bridge, but the span becomes clinically significant — a longer bridge places greater load on the abutment teeth and is more susceptible to failure. The maximum practical span for a conventional bridge is typically three or four teeth. Beyond this, implant support within the span is usually recommended.
✅ Quick Tip: Questions to Ask at Your Consultation
- What is my bone volume in the area of the missing tooth — and would I need grafting before an implant?
- Are my adjacent teeth healthy and unrestored, or already crowned? (This changes the bridge calculation significantly.)
- If I start with a denture now, can I upgrade to an implant later — and would bone grafting be needed at that point?
- What does each option cost in total over ten years, including maintenance and likely replacement?
- For my specific bite and the position of the missing tooth, which option gives the best long-term prognosis?
What It Is Like to Live With Each Option
Living With an Implant
Once fully healed and crowned, a dental implant requires no special care beyond normal brushing, flossing, and regular dental check-ups. Patients consistently report that they stop thinking about it — it feels like a tooth. There is no removal, no adhesive, no restriction on food. Bite force is equivalent to natural dentition. The aesthetic result is the most stable long-term of the three options because bone preservation beneath the implant maintains the gum contour and facial profile.
Living With a Bridge
A well-made bridge feels and looks natural and functions effectively for most foods. The main daily adjustment is cleaning — standard flossing cannot pass under the bridge, so a floss threader, interdental brush, or water flosser is needed to clean beneath the pontic and at the margins of the abutment crowns. Patients who are diligent about this cleaning routine maintain their bridges well; those who are not are at significantly elevated risk of decay and gum disease at the margins. There are no dietary restrictions specific to a bridge, but very hard foods that risk fracturing a crown apply equally here.
Living With a Denture
Adapting to a denture — particularly a first full denture — takes time. Speech is commonly affected in the first few weeks as the tongue and lips adjust. Eating requires adaptation: very hard, crunchy, or sticky foods are typically avoided. Partial dentures with clasps can feel bulky initially. Conventional dentures (without implant retention) may move during eating, which some patients find manageable and others find significantly disruptive to quality of life. The nightly removal and cleaning routine is an adjustment that most patients accommodate, though it remains a distinction from fixed options throughout.
Frequently Asked Questions
FAQ 1: Can I upgrade from a denture to implants later?
Yes, in most cases — but the timing matters. Bone resorption begins immediately after tooth loss and continues beneath a denture. The longer a gap has been present without a root replacement, the more bone may have been lost. Upgrading from a denture to implants may therefore require bone grafting that would not have been necessary if the implant had been placed earlier. If implants are your long-term goal and you are starting with a denture for financial or clinical reasons, discuss this plan with your dentist from the outset — they can make decisions about the denture design that preserve future implant options. For a full assessment, a consultation at Nova Dental Hospital including a CBCT scan gives a precise picture of current bone volume.
FAQ 2: Does getting a dental implant hurt?
Implant placement is carried out under local anaesthesia, which numbs the area completely. The procedure involves pressure and movement but should not be painful during the appointment. Post-operative soreness for two to five days after placement is normal — typically managed with over-the-counter pain relief and, in some cases, prescribed antibiotics to prevent infection. Most patients report that the recovery is more manageable than they anticipated. The pre-implant assessment at Nova Dental Hospital includes a CBCT 3D scan which allows precise surgical planning and reduces operative time.
FAQ 3: How long do dental implants last compared to bridges?
A dental implant, properly placed and maintained, has an expected lifespan of twenty or more years — with many cases lasting a patient’s lifetime. The crown on the implant may need replacement after fifteen to twenty years due to normal wear, but the implant fixture itself typically remains permanently integrated. A dental bridge lasts approximately ten to fifteen years before the cement seals begin to degrade, the porcelain wears or chips, or the underlying teeth develop problems that require attention. Each bridge replacement cycle involves further preparation of the abutment teeth.
FAQ 4: I am missing several teeth across the arch. Is a full implant solution realistic?
Yes, and it is the treatment that has transformed outcomes for patients with multiple missing teeth. A full-arch implant-supported bridge (All-on-4 or All-on-6) provides a complete fixed arch of teeth on four to six implants — eliminating the need for individual implants for each missing tooth and delivering a fixed, non-removable result at a significantly lower cost than individual implants for every position. For patients who want some implant stability without the cost of a fully fixed solution, an implant-retained overdenture is an effective middle option. Both approaches are planned as part of full mouth rehabilitation at Nova Dental Hospital.
FAQ 5: Which option is best for a missing front tooth?
For a single missing front tooth in a patient with adequate bone, a dental implant is the preferred option in most cases. The aesthetic result is the most stable long-term — the implant preserves the bone and gum contour that gives the front tooth its natural appearance. A bridge is a viable alternative if the adjacent teeth are already crowned or if implant surgery is not appropriate, but the eventual bone resorption beneath the pontic can create a visible gap at the gum line over time — which is more noticeable in the front of the mouth than in the back. A partial denture for a single front tooth is rarely the first choice for aesthetic reasons, though it may serve as a temporary solution. You are welcome to read about patient experiences at Nova Dental Hospital on our Google profile, where implant cases are among the most commonly reviewed treatments.
🔑 Key Takeaways
- Dental implants are the only option that replaces the tooth root, preserves the jawbone, and has no effect on adjacent teeth. They carry the highest upfront cost but typically the best long-term value and function.
- Dental bridges are fixed, non-surgical, and completed quickly — but require the permanent preparation of adjacent healthy teeth and do not prevent bone resorption beneath the gap.
- Dentures are the most accessible option initially, particularly for multiple or full-arch tooth loss, but require the most ongoing adjustment and provide the least stability and biting force without implant support.
- Implant-supported options — whether a fixed bridge or a clip-on overdenture — represent the most significant functional upgrade available for patients with multiple missing teeth.
- The right choice depends on bone volume, the condition of adjacent teeth, the number of missing teeth, general health, lifestyle, and how the patient weighs upfront cost against long-term value. No single answer applies to everyone.
- An accurate assessment requires clinical examination and imaging. A CBCT scan is the standard diagnostic tool for implant planning and gives both the patient and the clinician the most reliable picture of what is possible.
Conclusion: Three Good Options — One Best Option for Your Situation
Dental implants, bridges, and dentures have each been developed, refined, and validated over decades of clinical use. All three can restore appearance and function after tooth loss. The differences lie in what happens to the bone, what happens to adjacent teeth, how the restoration performs over twenty years, and how much management it requires along the way.
The honest summary is this: for most patients with a single or small number of missing teeth and adequate bone, a dental implant is the option that most closely replicates what was lost — in biology, function, aesthetics, and longevity. A bridge is a well-established alternative for patients where the adjacent teeth are already compromised or where surgery is not appropriate. Dentures serve an important role for patients with multiple missing teeth, limited bone, or limited budget — and in their implant-retained form, they deliver a significant step up in quality of life over a conventional plate.
The decision is always case-specific. At Nova Dental Hospital, every missing-tooth patient receives a full assessment — clinical examination, 3D CBCT imaging where indicated, and an honest conversation about what each option involves for their particular anatomy and circumstances. If you are weighing your options, a consultation is the right first step.
Related posts


Write a Comment
Recent Posts




