
Can a Cracked Tooth Be Saved, or Does It Have to Come Out?

Can a Cracked Tooth Be Saved, or Does It Have to Come Out?
The Problem With Cracked Teeth: They Are Easy to Ignore
A cracked tooth is one of the more clinically challenging problems in dentistry — not because the treatment options are complicated, but because the crack is often invisible. It does not always show on an X-ray. It may not cause constant pain. The patient may notice a sharp sensation when biting on something hard, or a brief sting with something cold, and then nothing — leading them to assume the problem has resolved on its own, or that it is not serious enough to act on.
Neither assumption is safe. A crack that is not assessed and managed progresses — slowly or suddenly, depending on the forces placed on the tooth. What begins as a crack confined to the crown of the tooth can extend into the root over weeks or months. What was a treatable fracture requiring a crown becomes a split tooth requiring extraction. The clinical window for saving a cracked tooth is real, and it closes.
This blog explains the different types of tooth fractures, the symptoms that suggest a crack is present, how they are diagnosed, what treatment is appropriate at each stage, and — critically — which cracks can be saved and which cannot. The aim is to give patients the information they need to act quickly enough that the most straightforward treatment option remains available.
🔑 Key Takeaways
- Not all cracked teeth are the same. The type, location, and depth of the crack determine whether the tooth can be saved and what treatment is required.
- Many cracked teeth produce intermittent rather than constant symptoms — a sharp pain on biting, brief cold sensitivity, or occasional discomfort that seems to come and go. This pattern is characteristic and should prompt a dental assessment, not a wait-and-see approach.
- Cracked tooth syndrome — a crack in the crown of the tooth that has not yet reached the root — is treatable with a crown in most cases. The sooner the crown is placed, the better the outcome.
- A vertical root fracture — a crack that runs along the root — cannot be treated and is the endpoint that leads to extraction. Preventing a crown fracture from progressing to a root fracture is the goal of early intervention.
- Bruxism (teeth grinding) is one of the most significant causes of cracked teeth. A cracked tooth in a patient who grinds should always prompt a conversation about night guard protection for the remaining teeth.
- Timing matters more for cracked teeth than almost any other dental problem. A tooth that is saveable today may not be saveable in six months.
The Five Types of Tooth Fracture — and Why the Distinction Matters
Dental fractures are not a single category. The classification system used clinically distinguishes five types, each with different implications for treatment and prognosis. Understanding these types helps patients understand why two people with a “cracked tooth” can have very different clinical situations.
| Fracture Type | What It Is | Symptoms | Can It Be Saved? | Typical Treatment |
| Craze Lines | Superficial cracks in the outer enamel only — very common in adult teeth, visible as fine lines on the tooth surface | Usually none — cosmetic finding only | Yes — no treatment needed | Monitoring only; no intervention required |
| Fractured Cusp | A cusp (the raised point of a back tooth) breaks off, usually around a large filling | Sudden relief of previous discomfort; rough edge; sensitivity | Yes — usually straightforward | Crown or large filling to restore the tooth |
| Cracked Tooth (Cracked Tooth Syndrome) | A crack extending from the biting surface downward into the tooth — may or may not reach the pulp | Sharp pain on biting; brief cold sensitivity; pain difficult to localise | Yes — if caught before reaching the root | Crown; root canal if pulp is involved; prognosis worsens as crack deepens |
| Split Tooth | A crack has progressed fully through the tooth, dividing it into two separate segments | Severe pain; visible fracture; tooth may feel mobile | Sometimes — depends on crack position | Extraction of one segment; possible retention of the other if anatomy allows; often full extraction |
| Vertical Root Fracture | A crack running along the length of the root — typically originating from inside the root, often in root-canal-treated teeth | Often minimal — localised gum swelling, mild ache, recurrent abscess around one tooth | No — extraction required | Extraction; implant or bridge for replacement |
The clinical significance of this classification is that it maps directly to treatment options. Craze lines are a cosmetic finding. A fractured cusp is usually straightforward to manage. A cracked tooth — the type responsible for cracked tooth syndrome — is the clinically important category where timing is critical: caught before the crack reaches the root, it is treatable; allowed to progress to a vertical root fracture, it is not. This is the decision window that early assessment protects.
Recognising the Symptoms: What a Cracked Tooth Feels Like
The symptom pattern of a cracked tooth is one of the most distinctive — and one of the most commonly misread — in dentistry. The classic presentation of cracked tooth syndrome involves three characteristics that, taken together, should prompt immediate assessment:
1. Sharp Pain on Biting — Especially on Release
The hallmark of a cracked tooth is a sharp, brief pain that occurs when biting down on something — particularly something hard or crunchy — and is often more pronounced on the release of biting pressure rather than at the moment of contact. This rebound pain occurs because the biting force briefly opens the crack, and the release allows it to close again, stimulating the nerve tissue inside the tooth. The pain is usually sharp and transient — it lasts a second or two and then fades — rather than a lingering ache.
Patients often describe being able to reproduce the pain by biting on a specific area of the tooth, or by chewing on a specific side of the mouth. This reproducibility is useful clinically — it suggests a structural rather than an inflammatory cause.
2. Brief, Sharp Cold Sensitivity
Cold sensitivity — a brief, sharp pain triggered by cold drinks or food — is another common feature of a cracked tooth. Unlike the diffuse cold sensitivity of exposed dentine (which affects multiple teeth and is more of a dull ache), the cold sensitivity of a cracked tooth is usually localised to one tooth and is sharp and brief in character. Heat sensitivity, when present, suggests the pulp has become inflamed or infected — a sign that the crack has allowed bacteria to reach the inner tooth.
3. Intermittent Rather Than Constant Pain
This is the feature that most often leads to delayed treatment. Unlike a toothache from decay or an abscess — which tends to be persistent, escalating, and impossible to ignore — the pain from a cracked tooth is intermittent. It comes when provoked by biting or cold, and disappears between stimuli. Many patients interpret this as the problem resolving, or as not serious enough to act on. It is neither. The intermittent nature simply reflects the mechanical character of the problem — the crack opens under load and closes at rest. The underlying fracture is not healing.
Symptoms That Suggest the Crack Has Progressed
If any of the following symptoms develop alongside or after the characteristic cracked tooth pain pattern, they suggest the crack has deepened and the pulp may be involved or infected — prompting more urgent assessment:
- Spontaneous pain — toothache that occurs without biting or cold stimulus
- Prolonged sensitivity to heat — hot drinks causing lingering pain
- Visible swelling in the gum next to the tooth
- A persistent bad taste — suggesting infection draining from around the root
- The tooth feeling loose or mobile
⚠️ Seek Assessment Promptly If You Notice:
- Sharp pain when biting, particularly on release of pressure — especially if it can be reproduced on the same tooth consistently
- Brief sharp cold sensitivity in one specific tooth with no obvious cause (no visible decay, no recent dental work)
- Any of the above that has been present for more than a few days without improvement
- A sudden crack or crunch sensation when biting, even if the pain subsides — a cusp may have fractured and a fragment may still be in place
How a Cracked Tooth Is Diagnosed
Diagnosing a cracked tooth is one of the more technically demanding assessments in general dentistry. The crack is often not visible to the naked eye and does not always show on a conventional X-ray — particularly in its early stages, when the crack runs vertically and the X-ray beam cannot be aligned to show it as a dark line.
Clinical Examination
The dentist will examine the tooth closely under good lighting — ideally with magnification — looking for any visible crack lines on the crown surface or between the cusps. Staining the tooth with a dye (such as methylene blue) can make fine crack lines visible by penetrating and highlighting them. Transillumination — shining a bright light through the tooth from behind — can also reveal cracks as dark lines that interrupt the light transmission.
Bite Test
A bite test using a small plastic stick or dedicated bite testing device (a Tooth Slooth) reproduces the biting pain by allowing the patient to bite on individual cusps selectively. By identifying which cusp position reproduces the pain, the dentist can locate the crack and estimate its extent. This is often the single most useful diagnostic tool for cracked tooth syndrome — it uses the patient’s own symptoms to identify the crack location precisely.
Periodontal Probing
A thin periodontal probe is run around the gum margin of the tooth. If the crack has extended into or below the gum line, the probe drops into a narrow, isolated deep pocket adjacent to the crack — a characteristic finding that indicates a subgingival crack extension. This finding significantly affects the prognosis of the tooth and the treatment options available.
CBCT 3D Imaging
In complex cases — where the extent of the crack is unclear from clinical examination, or where a root fracture is suspected — a CBCT 3D scan provides the most detailed imaging available. A CBCT scan can visualise the root in three dimensions and detect crack-related changes in the surrounding bone that are invisible on a conventional two-dimensional X-ray. It is particularly useful for identifying vertical root fractures and for assessing the depth of a crack relative to the bone level — information that directly influences whether extraction or a more conservative approach is appropriate.
Vitality Testing
Testing whether the tooth’s pulp is alive — by applying cold or a small electrical stimulus to the tooth surface — gives information about whether the pulp has already been damaged by the crack. A tooth whose pulp has died (negative vitality response) will need root canal treatment as part of the management, regardless of whether a crown can still save the structure. A tooth with a vital pulp that is not yet inflamed has the most favourable prognosis.
The Treatment Decision Tree: From Monitoring to Extraction
Once the type and extent of the crack have been established, the treatment pathway follows a clear decision tree. The key question at each branch is the same: does the crack remain within the saveble range, or has it crossed the line into irreparable territory?
Craze Lines — Monitoring Only
Craze lines are cosmetic and clinically insignificant. They do not require treatment. The dentist will note them and monitor at routine check-ups to ensure they are not associated with any structural symptoms. No intervention is needed.
Fractured Cusp — Crown or Restoration
A fractured cusp that has broken away from the tooth removes the immediate cause of discomfort (the mobile cusp was the source of the biting pain) but leaves the remaining tooth structure at risk of further fracture. The standard management is a crown to bind the remaining tooth structure and prevent further cracking. If the fracture has exposed the pulp, root canal treatment is needed before crowning. Fractured cusps that are managed promptly — before the remaining structure cracks further — have a good prognosis.
Cracked Tooth Syndrome — Crown, With or Without Root Canal
This is the clinically critical category — and the one where timing has the most impact. A crack that extends from the biting surface downward but has not yet reached the root is managed with a crown. The crown encircles the entire tooth, preventing the crack from opening under biting load and halting its progression. The crown does not repair the crack — the crack remains — but it eliminates the mechanical force that was driving the crack deeper.
Whether root canal treatment is needed alongside the crown depends on the condition of the pulp. If the pulp is vital and not significantly inflamed, the crown alone may be sufficient. If the pulp is already inflamed (irreversible pulpitis — indicated by spontaneous pain or prolonged heat sensitivity) or has died, root canal treatment is performed before the crown is placed.
The prognosis of a cracked tooth treated with a crown is good if the crack has not reached the root — studies report survival rates of around 85 to 90 percent at five years for appropriately selected cases. The prognosis worsens significantly if the crack has extended below the level of the bone, or if there is a deep periodontal pocket associated with the crack. This is why assessment timing matters: the same tooth that has an excellent prognosis today may have a guarded prognosis in three months if the crack has progressed.
Split Tooth — Partial Retention or Extraction
A split tooth — where the crack has progressed through the full width of the tooth, dividing it into two distinct segments — presents a different clinical picture. In most cases, the tooth cannot be saved in its entirety. However, if the crack runs in a favourable direction and one segment retains adequate root support and bone attachment, it may be possible to extract the unsalvageable segment and retain the other half, restoring it with a crown. This is uncommon and applies only to specific anatomical situations — most split teeth require full extraction.
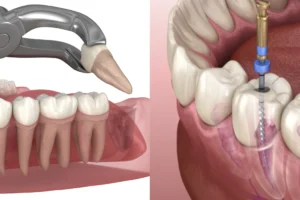
Vertical Root Fracture — Extraction
A vertical root fracture — a crack running along the length of the root — has no restorative solution. The fracture creates a pathway for bacterial contamination along the full length of the root, causing progressive bone loss around the root that cannot be halted by any treatment short of removing the tooth. Extraction is the only clinical option. Following extraction, the gap is managed with a dental implant, bridge, or denture as appropriate — a process covered in detail in our blog on implants vs dentures vs bridges.
Vertical root fractures most commonly occur in teeth that have had root canal treatment — the root canal procedure, particularly if the root was over-prepared or if a post was placed, can weaken the root structure and predispose it to longitudinal cracking under biting load. This is one of the reasons why crown protection after root canal treatment is so important — the crown reduces the biting forces transmitted to the root and significantly lowers the risk of vertical root fracture.
| Crack Type | Can It Be Saved? | Treatment | Key Timing Consideration |
| Craze Lines | Yes — no treatment needed | Monitor only | No urgency — cosmetic finding |
| Fractured Cusp | Yes — usually straightforward | Crown ± root canal | Prompt treatment prevents further fracture |
| Cracked Tooth (above root) | Yes — if treated before crack reaches root | Crown ± root canal | Critical window — delay worsens prognosis significantly |
| Split Tooth | Sometimes — one segment may be retained | Partial or full extraction; crown if segment retained | Usually presents as an acute event — seek same-day assessment |
| Vertical Root Fracture | No | Extraction + replacement planning | Extraction timing affects bone volume for future implant |
What Causes Teeth to Crack?
Understanding the causes of tooth fractures helps patients identify whether they are at elevated risk — and whether there is anything they can do to reduce that risk for remaining teeth.
Bruxism — Teeth Grinding and Clenching
Bruxism is one of the most significant risk factors for cracked teeth. As discussed in our blog on bruxism, headaches, and jaw pain, the forces generated during sleep grinding can reach three to four times normal biting force — sustained across hundreds of events per night. This repeated high-force loading on the tooth structure is a primary driver of fatigue cracking, particularly in back teeth. A patient who presents with a cracked tooth and is also a known or suspected grinder should always be assessed for bruxism and considered for a night guard to protect the remaining teeth.
Large Fillings
Teeth with large fillings — particularly old amalgam fillings that have been in place for many years — are at significantly elevated risk of cracking. A large filling removes a substantial portion of the tooth’s internal structure, leaving the remaining cusps as relatively thin, unsupported walls that are vulnerable to fracture under normal biting load. This is one of the clinical reasons why back teeth with very large fillings are often recommended for crowns even before a fracture occurs — the crown binds the remaining cusps and prevents the fracture that is otherwise increasingly likely.
Biting on Hard Objects
Cracking a tooth on an unexpected hard object — an olive stone, an unpopped popcorn kernel, a bone fragment — is a common cause of acute fracture. The tooth structure, which can withstand the distributed forces of normal chewing, is not designed for the sudden concentrated force of biting something unexpectedly hard. This type of fracture is not entirely preventable, but patients who regularly crack their teeth on hard foods or habitually chew hard objects (ice cubes, pens) are at elevated risk.
Thermal Stress
Repeated rapid temperature changes — drinking hot coffee immediately followed by cold water — can contribute to craze line formation and, over time, to deeper cracking. The enamel and dentine expand and contract at slightly different rates with temperature change, and repeated cycling of this stress creates microscopic fracture lines. This is a contributing factor rather than a sole cause in most cases.
Trauma
A direct blow to the face — from sports, an accident, or a fall — can fracture teeth acutely. Trauma-related fractures can range from minor enamel chipping to complete crown fractures and root fractures. Any tooth that has been subjected to significant trauma should be assessed promptly, even if there is no immediate pain, as the pulp can be damaged without external structural evidence being visible.
Previous Root Canal Treatment
Root canal-treated teeth are at elevated risk of vertical root fracture for the reasons outlined above — the removal of the pulp tissue reduces internal moisture and slightly increases brittleness, and certain root canal techniques or post placements can weaken the root. This is the strongest argument for placing a crown promptly after root canal treatment rather than leaving the tooth uncrowned for an extended period.
What to Do If You Think You Have a Cracked Tooth
The most important action is to have it assessed promptly. As this guide has outlined, the treatment options and prognosis for a cracked tooth are directly linked to how much the crack has progressed — and progression continues whether or not the tooth is symptomatic between biting events.
✅ Practical Steps While Awaiting Your Appointment
- Avoid biting on the affected side — reduce the load on the suspected cracked tooth to slow progression.
- Avoid very hot and very cold food or drinks — temperature extremes will aggravate the symptoms and provide no clinical benefit.
- Do not attempt to assess the crack yourself — running a fingernail or object along the tooth does not give useful information and risks displacing a fragment that is holding the crack together.
- Note which actions reproduce the pain — specific information about whether the pain occurs on biting down or on release, on cold or heat, and on which side of the mouth is useful diagnostic information for your dentist.
- Seek same-day assessment for acute fractures — if you felt or heard a crack while eating, and particularly if there is sharp pain or a visible fragment, contact the clinic for a same-day appointment rather than waiting.
At Nova Dental Hospital, cracked tooth assessment includes clinical examination with bite testing, transillumination, and periodontal probing, supplemented by CBCT imaging where the clinical picture is uncertain. A general dentistry consultation is the appropriate starting point — and the sooner it happens, the more treatment options remain available.
Frequently Asked Questions
FAQ 1: My cracked tooth does not hurt all the time. Does that mean it is not serious?
No — intermittent pain is the characteristic symptom of cracked tooth syndrome, not a sign that the problem is minor. The pain is provoked by biting and cold because the crack opens and closes under mechanical and thermal load. Between these triggers, the tooth may feel completely normal. This intermittent pattern is one of the reasons cracked teeth are often left too long before assessment. The crack is not healing during the pain-free intervals — it is simply at rest. A tooth that produces sharp biting pain consistently when loaded on a specific area should be assessed regardless of whether it hurts at other times.
FAQ 2: Can a tooth crack under a crown?
Yes. A crown protects the visible portion of the tooth and reduces the forces transmitted to the crown structure — but it does not fully protect the root. A vertical root fracture can develop in a crowned tooth, typically originating from inside the root canal if the root has been over-prepared or if a post and core has placed uneven stress on the root walls. This is why regular dental check-ups remain important even for crowned teeth — the crown can be examined for signs of margin breakdown, and the gum tissue around the tooth can be probed for the narrow isolated pockets that suggest a subgingival crack.
FAQ 3: I grind my teeth at night. Am I at higher risk of cracked teeth?
Yes — significantly so. Bruxism generates forces three to four times higher than normal biting load and applies them repeatedly across hundreds of grinding events per night. This sustained high-force cycling is a primary driver of dental fatigue cracking, particularly in the back teeth which bear the highest loads. If you are a known grinder with back teeth that have large fillings or that have had root canal treatment, the risk of fracture is elevated enough that your dentist may recommend crowning those teeth proactively — before a crack develops — rather than waiting. A night guard, as discussed in our blog on bruxism and jaw pain, reduces the forces reaching the teeth during grinding and is an important protective measure.
FAQ 4: How long does treatment for a cracked tooth take?
For a cracked tooth managed with a crown alone — where the pulp is vital and uninvolved — the treatment involves two appointments: a preparation appointment (tooth shaped, impression or scan taken, temporary crown placed) and a fit appointment approximately one to two weeks later when the permanent crown is ready. If root canal treatment is needed before the crown — because the pulp is inflamed or has died — this adds one to two appointments before the crown preparation, typically extending the total treatment to three to four appointments over three to four weeks. Extraction, if required, is typically completed in one appointment, with replacement planning beginning after the socket has healed.
FAQ 5: What happens if I leave a cracked tooth untreated?
The crack will progress — gradually under normal biting load, or suddenly if significant force is applied. A crack confined to the crown that could have been saved with a crown will extend into the root and become a split tooth or vertical root fracture, at which point extraction is the only option. The longer the crack is left, the higher the probability of reaching this irreversible endpoint. Additionally, a crack that has penetrated the pulp without being treated will lead to pulp infection and abscess — adding the complications of infection to the structural problem. If you suspect a cracked tooth, a prompt assessment at Nova Dental Hospital gives you the most accurate picture of where the crack is and what options are available. Patients are also welcome to share their experience on our Google Business Profile.
🔑 Key Takeaways
- Cracked teeth exist on a spectrum from cosmetic craze lines to unsalvageable vertical root fractures. The position on that spectrum — and the treatment options available — depends almost entirely on how deep the crack has progressed.
- Cracked tooth syndrome produces a characteristic pattern: sharp pain on biting (especially on release), brief cold sensitivity, and intermittent rather than constant symptoms. This pattern should prompt assessment, not watchful waiting.
- A crown is the standard treatment for a cracked tooth that has not yet reached the root. It halts crack progression and, in most cases, allows the tooth to function normally for many years. Root canal treatment is added if the pulp is already compromised.
- Vertical root fractures cannot be repaired and require extraction. The goal of early intervention is precisely to prevent a treatable crown fracture from progressing to an untreatable root fracture.
- Bruxism is a major risk factor for cracked teeth. Patients who grind their teeth — particularly those with large fillings or root-canal-treated back teeth — should discuss night guard protection and proactive crown placement with their dentist.
- Timing is the variable the patient controls. The sooner a cracked tooth is assessed, the more treatment options remain available and the better the prognosis.
Conclusion: Whether a Cracked Tooth Can Be Saved Depends on You Acting Promptly
The frustrating truth about cracked teeth is that the answer to the question — can it be saved? — is often determined not by the crack itself, but by when the patient has it assessed. A crack that is treatable with a straightforward crown appointment today may become non-restorable in three months if it progresses unchecked to the root.
The biology of tooth fracture is unforgiving in one specific way: cracks do not heal. They progress. The window for the most conservative treatment — a crown, without root canal, with a good long-term prognosis — is open for a finite time. Once the crack crosses below the level of the bone, or once the root is involved, that window closes permanently.
If you have noticed a sharp pain when biting on a specific tooth, brief cold sensitivity that seems localised, or felt or heard a crack while eating, the right response is a prompt dental assessment — not a wait-and-see approach. At Nova Dental Hospital, cracked tooth cases are assessed with bite testing, transillumination, and 3D imaging where needed, so the clinical picture is complete before any treatment decision is made. The earlier you come in, the more options remain on the table.
Related posts


Write a Comment
Recent Posts




