
Root Canal vs Tooth Extraction: Which Is Actually the Better Choice?
Root Canal vs Tooth Extraction: Which Is Actually the Better Choice?
The Question Every Patient With a Painful Tooth Eventually Asks
There is a moment in the dental chair when a patient learns their tooth is severely infected or badly damaged, and they face a decision that feels impossible to make with confidence. The dentist has explained two options — a root canal treatment to save the tooth, or an extraction to remove it — and the patient is trying to work out which is cheaper, which is quicker, which hurts less, and which is the smarter long-term call.
This decision comes up repeatedly, and the same misunderstanding drives most of the uncertainty. The assumption — usually unstated but almost universal — is that extraction is the simpler, cheaper, more decisive option. Pull the tooth, problem solved, move on.
The clinical reality is considerably more complicated. Extraction is not the end of the story — it is the beginning of a different and often more expensive one. This blog explains how the decision between a root canal and an extraction is actually made, what each option involves, what the genuine long-term implications are, and how to approach the conversation with your dentist with the right questions.
🔑 Key Takeaways
- Root canal treatment saves the natural tooth by removing infected or damaged pulp tissue, sealing the root canals, and restoring the tooth with a crown. The tooth remains functional in the jaw.
- Extraction removes the tooth entirely — and almost always creates a gap that needs to be managed, either with an implant, a bridge, or a denture. These are additional procedures, additional cost, and additional treatment time.
- The cost of extraction is rarely just the extraction. When the full replacement pathway is costed realistically, saving the tooth with a root canal is often the more economical option over any meaningful time horizon.
- A natural tooth — even one that has had a root canal — generally outperforms any replacement for function, feel, and bone preservation. The goal of dentistry is always to keep natural teeth where clinically possible.
- The decision depends on clinical factors: the tooth’s restorability, the extent of bone loss, the root anatomy, and the patient’s overall oral health. It is not a generic choice — it is case-specific.
What Root Canal Treatment Actually Involves
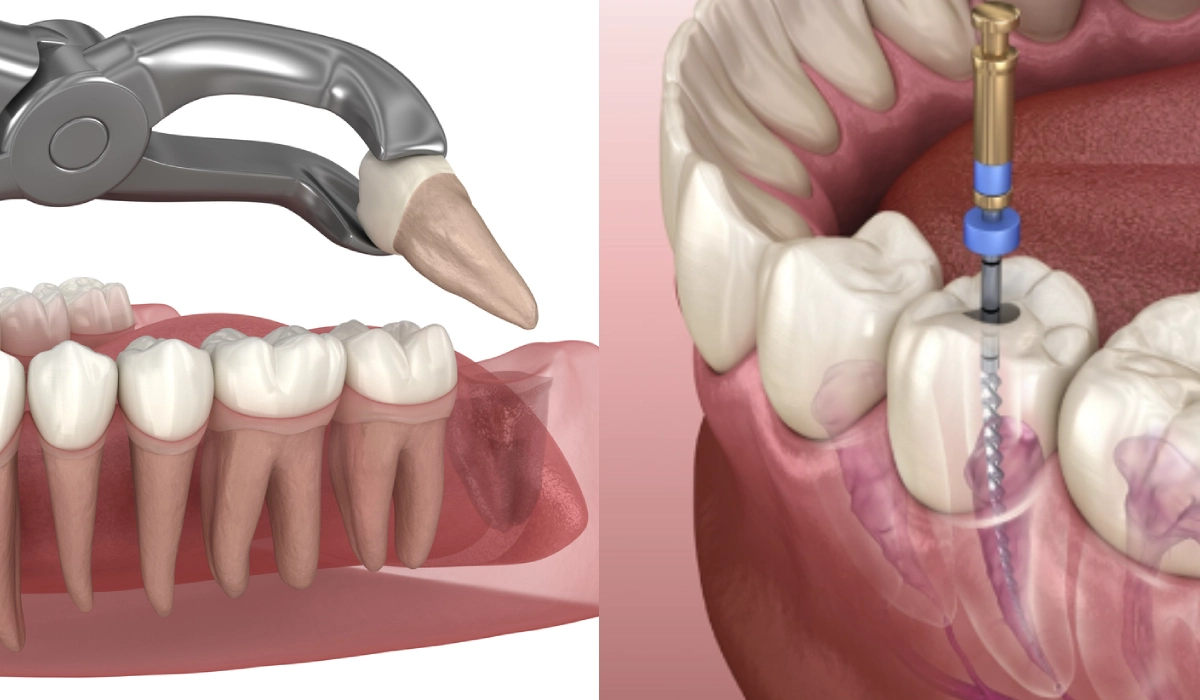
Root canal treatment — formally called endodontic treatment — is the process of removing the infected or inflamed tissue from inside a tooth, cleaning and shaping the root canal system, and sealing it permanently. The tooth is then typically restored with a crown to protect it from fracture under biting forces.
The procedure addresses the source of the infection — the pulp tissue that has become infected, usually because of deep decay, a crack, or trauma — without removing the tooth itself. Once the pulp is removed and the canals are cleaned and sealed, the tooth is no longer alive in the biological sense, but it remains firmly anchored in the jaw, fully functional, and indistinguishable from adjacent teeth once restored.
What the Procedure Involves, Step by Step
- Local anaesthesia: The tooth and surrounding tissue is numbed. A well-administered local anaesthetic means the procedure itself should not be painful — the expectation of pain during a root canal is largely historical, from an era before modern anaesthesia techniques.
- Access opening: A small opening is made through the top of the tooth to reach the pulp chamber.
- Pulp removal and canal shaping: The infected pulp tissue is removed using fine instruments. The root canals are shaped and cleaned with irrigating solutions that eliminate bacteria.
- Canal filling: The cleaned canals are filled with a biocompatible material called gutta-percha, which seals the space and prevents reinfection.
- Restoration: In most cases — particularly for back teeth that bear significant chewing loads — the tooth is subsequently crowned. A crown protects the now-brittle tooth from fracture and restores full function.
The number of appointments required depends on the complexity of the case. Straightforward front teeth with a single canal may be completed in one appointment. Molar teeth, which typically have three or four canals and more complex anatomy, often require two appointments. At Nova Dental Hospital, painless root canal treatment is carried out using modern rotary instrumentation and magnification where indicated, which improves both thoroughness and patient comfort considerably.
When Root Canal Treatment Is the Right Choice
- The tooth has sufficient healthy structure remaining to be restorable — enough crown and root to support a permanent restoration.
- The surrounding bone is intact or only minimally affected — significant bone loss around the root changes the prognosis.
- The root canals are accessible and negotiable — heavily calcified or unusually curved canals can complicate the procedure, though specialist techniques address most anatomical challenges.
- The patient wants to keep their natural teeth — which, all else being equal, is always the clinically preferred outcome.
What Tooth Extraction Involves — and What Comes After
An extraction is the surgical removal of a tooth from its socket. For straightforward erupted teeth, this is a relatively quick procedure under local anaesthesia. For teeth with curved or multiple roots, heavily broken-down structure, or proximity to nerves and sinuses — as is common with lower wisdom teeth — the procedure is more involved and may require sectioning the tooth or careful elevation of surrounding bone.
The extraction itself is not the difficult part of this decision. The difficult part is what comes after the extraction, and whether the patient has fully accounted for it.
The Gap Left by an Extracted Tooth Is Not Neutral
This is the most important thing patients do not fully appreciate when they choose extraction. A missing tooth does not leave a benign empty space. Within weeks and months of extraction, a predictable chain of biological events begins:
- Bone resorption: The jawbone that surrounded the tooth root begins to shrink. In the first year after extraction, approximately 25 percent of bone width is lost. Over subsequent years, further resorption continues. This bone loss is permanent without intervention.
- Adjacent and opposing tooth movement: Without a neighbour to bear against, adjacent teeth tilt into the space over time. The opposing tooth — the one that bit against the extracted tooth — begins to over-erupt, moving out of the gumline towards the gap. This disrupts the bite and can eventually compromise both adjacent teeth.
- Bite changes and jaw joint load: As the bite shifts to compensate for the missing tooth, load distribution across the remaining teeth changes. Over years, this contributes to accelerated wear on other teeth and can increase the load on the jaw joint.
- Aesthetic changes: Bone loss beneath the gum alters the facial profile over time. The cheek or lip in the area of extraction gradually loses support. For front teeth especially, the aesthetic consequence is significant.
None of these consequences are hypothetical. They are predictable, well-documented, and the reason why extraction — despite appearing to resolve the immediate problem quickly — so often becomes the beginning of a longer and more expensive treatment journey.
Replacing the Extracted Tooth: The Real Cost Equation
For any tooth other than a third molar (wisdom tooth), a gap should be managed with a replacement. The three main options are:
| Replacement Option | How It Works | Bone Preservation | Key Consideration |
| Dental Implant | A titanium fixture is placed in the jawbone and topped with a crown. Functions and feels like a natural tooth. | Yes — the implant stimulates the bone and prevents resorption | The closest equivalent to a natural tooth. Requires adequate bone volume; if significant resorption has already occurred, bone grafting may be needed before placement. |
| Dental Bridge | A fixed prosthetic that spans the gap by crowning the adjacent teeth on either side and suspending an artificial tooth between them. | No — bone beneath the gap continues to resorb without a root | Involves cutting down two healthy adjacent teeth to serve as bridge abutments. Once cut, those teeth require crowning for life. |
| Removable Denture (Partial) | A removable acrylic plate with artificial teeth, retained by clasps on adjacent teeth. | No — bone resorption continues beneath the denture | Least expensive initially but least functional. Requires adjustment as the bone ridge changes shape over time. |
| No Replacement | Leave the gap unmanaged. | No — resorption proceeds unchecked | Only clinically acceptable for third molars that do not affect bite function. For all other teeth, not replacing creates the cascade of movement and bone loss described above. |
The financial reality of extraction followed by implant placement — particularly if bone grafting is required due to delayed placement — is frequently higher than the cost of root canal treatment plus a crown on the original tooth. Patients who choose extraction on cost grounds and then pursue implant replacement later often end up spending more than they would have spent preserving the tooth. Patients considering their options are always welcome to book a general dentistry consultation at Nova Dental Hospital for a full clinical assessment and honest cost comparison for their specific situation.
How the Clinical Decision Is Actually Made
The choice between root canal treatment and extraction is not made generically — it is made case by case, based on a set of clinical factors that the dentist evaluates at examination. Understanding these factors helps patients follow the reasoning and ask the right questions.
Restorability of the Tooth
The central question in any root canal decision is whether the tooth is restorable — whether there is enough healthy tooth structure remaining to support a crown after the root canal is completed. A tooth that has been severely broken down by decay, has a fracture extending below the gum line, or has insufficient root support may not be predictably restorable even if the root canal itself is technically successful. If the restoration is likely to fail, the tooth may not be worth saving.
Radiographic assessment — including, in complex cases, a CBCT 3D scan — gives the dentist a clear picture of the remaining structure, root length, bone levels, and the relationship of the tooth to adjacent anatomy before committing to a treatment plan.
Degree of Bone Loss Around the Root
Significant bone loss around the root — whether from advanced gum disease, a dental abscess, or a vertical fracture — reduces the prognosis for root canal treatment. A tooth that is mobile because of extensive bone loss is unlikely to remain functional even after a technically successful root canal. In these cases, extraction followed by a planned replacement pathway may be the more realistic option.
Root Anatomy and Canal Complexity
Some teeth have straightforward, accessible canal systems that are well suited to routine root canal treatment. Others — particularly upper molars with curved or calcified canals, or lower molars with four or more canals — present a more complex anatomy. Modern rotary instrumentation and the use of dental operating microscopes in specialist settings have significantly increased the proportion of teeth that can be successfully treated, but anatomy still influences prognosis and, where relevant, the decision of whether to refer to a specialist endodontist.
The Patient’s Overall Oral Health Context
A tooth does not exist in isolation. A patient with multiple failing teeth, severe periodontal disease, or systemic health factors that complicate healing may need a treatment plan that addresses the whole mouth rather than one tooth at a time. In some cases, extraction is part of a broader restorative plan — for example, where a patient is planning a full arch restoration with implants and the tooth in question is not viable long-term. The decision is always made in the context of the complete clinical picture.
The Wisdom Tooth Exception
Third molars — wisdom teeth — are a specific exception to the general principle of saving natural teeth. Wisdom teeth that are impacted, difficult to keep clean, causing crowding or damage to adjacent teeth, or repeatedly infected are commonly extracted without replacement because they do not serve an essential function in most patients’ dentition. The bone resorption and movement consequences that apply to other extracted teeth are generally not clinically significant for third molars.
Root Canal vs. Extraction: A Direct Comparison
| Root Canal Treatment | Tooth Extraction | |
| What happens to the tooth | Tooth is saved and remains in the jaw | Tooth is permanently removed |
| Procedure pain (during) | Should be pain-free with adequate local anaesthesia | Should be pain-free with adequate local anaesthesia |
| Recovery | Mild soreness for a day or two; normal function quickly | Several days of soreness; socket healing over weeks |
| Bone preservation | Yes — root remains in jaw, bone maintained | No — bone resorption begins immediately after extraction |
| Adjacent tooth movement | No — natural tooth holds position | Yes — over time, adjacent and opposing teeth shift |
| Replacement needed | No — tooth remains | Usually yes — implant, bridge, or denture for most positions |
| Long-term function | Equivalent to natural tooth when properly crowned | Depends on replacement chosen; implant closest to natural |
| Number of appointments | Typically 2–3 (including crown) | 1 for extraction; additional for replacement |
| Longevity | Root canal teeth can last decades with proper restoration | Replacement longevity varies by type chosen |
| Best suited for | Teeth with salvageable structure and adequate bone support | Non-restorable teeth, advanced bone loss, third molars |
The Misconceptions That Lead Patients to the Wrong Decision
“Extraction is cheaper”
The extraction procedure itself may cost less than root canal treatment. But extraction is not the final cost — it is the first cost. For any tooth other than a wisdom tooth, the gap needs to be managed. A dental implant with a crown, or a bridge requiring the preparation of adjacent teeth, adds substantially to the overall cost. When the realistic full pathway is costed — extraction, socket healing, bone grafting if needed, implant, crown — the total frequently exceeds what root canal treatment and a crown on the original tooth would have cost.
“Root canals are extremely painful”
This is perhaps the most persistent myth in dentistry. Root canal treatment has a poor reputation that belongs to a previous era of dental anaesthesia and technique. Modern painless root canal treatment is carried out under effective local anaesthesia, and the procedure itself — once the area is adequately numb — is no more uncomfortable than having a filling placed. Patients who have experienced a root canal under modern conditions consistently report that the procedure was far less unpleasant than the tooth pain that preceded it. The fear of root canal pain is a significant driver of avoidable extractions.
“It’s just a tooth — I’ll manage without it”
Patients often underestimate how much they will notice a missing tooth — both functionally and aesthetically — until it is gone. Chewing efficiency shifts. The feel of the bite changes. If the gap is visible, confidence in smiling changes. And as adjacent and opposing teeth begin to drift over months and years, the consequences compound in ways that were not apparent at the time of the decision.
“The tooth is infected, so it has to come out”
Infection in a tooth does not mean the tooth must be extracted. It means the source of the infection — the infected pulp — needs to be addressed. Root canal treatment does precisely this: it removes the infected tissue, eliminates the bacteria, and seals the space so reinfection cannot occur. A tooth with a dental abscess can, in most cases, be successfully treated with a root canal and retained for many years.
✅ Quick Tip: Questions to Ask Your Dentist Before Making This Decision
- Is this tooth restorable? What is the prognosis after root canal treatment?
- If I extract this tooth, what are my replacement options and what is the realistic cost of each?
- How much bone is present around this tooth, and would that affect implant placement later?
- Are there any clinical reasons why root canal treatment is not recommended for this specific tooth?
- What happens if I delay making a decision — and for how long is that safe?
When Extraction Is the Right Answer
It would be misleading to suggest that root canal treatment is always the correct choice. There are clear clinical situations where extraction is the appropriate and recommended decision:
- Vertical root fracture: A crack that runs along the length of the root — rather than across the crown — cannot be repaired. A tooth with a confirmed vertical root fracture has a very poor prognosis regardless of root canal treatment and is typically best extracted.
- Severe bone loss to the apex: When bone loss has extended to the very tip of the root due to advanced periodontal disease or a longstanding abscess, the tooth has no functional support and cannot be maintained.
- Non-restorable crown: A tooth destroyed by decay or fracture to the point where there is insufficient structure to support a restoration, even with post and core build-up, cannot be saved by root canal treatment alone.
- Failed previous root canal with no retreatment option: Root canals can be retreated if an initial treatment fails, but if retreatment has also failed and surgical options are not feasible, extraction becomes the endpoint.
- Orthodontic extraction: In some orthodontic treatment plans, a tooth may be extracted to create space for correct alignment of the remaining teeth. This is a planned extraction with a specific clinical purpose.
- Wisdom teeth causing problems: Impacted, repeatedly infected, or structurally damaging wisdom teeth are extracted without replacement in most cases.
In these situations, the dentist’s recommendation of extraction is not a second-best outcome — it is the clinically appropriate decision based on the specific anatomy and condition of that tooth. The important principle is that the decision is made on clinical grounds, not on the basis of cost, time, or patient anxiety.
What to Expect If You Proceed With Root Canal Treatment
During the Procedure
Once the area is anaesthetised — which should take the sensation away completely — you will feel pressure and movement but not pain. The procedure involves working inside the tooth, and some patients find the sounds and sensations unfamiliar, but discomfort during a well-administered root canal is not the norm. The appointment typically lasts between 60 and 90 minutes for a straightforward case, longer for complex molar teeth.
After the Procedure
Mild soreness and tenderness in the treated tooth and surrounding gum for one to three days after the procedure is normal and expected. Over-the-counter pain relief is usually adequate to manage this. The tooth may feel slightly different to bite on for a few days while the inflammation around the root resolves. If significant pain develops or does not settle within a few days, contact the clinic — this is uncommon but warrants review.
Until the permanent restoration is placed — usually a crown — avoid chewing on the treated tooth with hard or sticky foods. The tooth is temporarily sealed after the root canal is completed and is more vulnerable to fracture before the crown is fitted.
The Crown Appointment
The root canal treatment is only complete once the tooth has been permanently restored. For most back teeth, this means a crown — a full-coverage ceramic or zirconia restoration that protects the tooth from fracture. At Nova Dental Hospital, dental crowns are matched to the shade of adjacent teeth and are indistinguishable in appearance from natural teeth. The crown appointment follows after the root canal, typically at a separate visit once the tooth has settled.
Frequently Asked Questions
FAQ 1: Can I wait to decide between root canal and extraction?
In some cases, a short delay while you consider your options is clinically acceptable — particularly if the tooth is not acutely painful and is not showing signs of spreading infection. However, dental infection does not pause while you decide. An untreated abscess can spread to surrounding bone and soft tissue, and a tooth that is borderline restorable today may become non-restorable if further decay or fracture progresses. In most cases, the sooner the decision is made, the more options remain open. If you are unsure, a consultation at Nova Dental Hospital will give you a clear clinical assessment and the time to ask all the questions you need before committing to either path.
FAQ 2: Is a root canal covered by dental insurance in India?
Coverage varies by plan. Basic dental insurance in India typically covers some portion of root canal treatment — particularly for anterior teeth — as it is classified as a restorative rather than cosmetic procedure. Molar root canals and the associated crown are more variably covered. Our blog on dental insurance and cosmetic coverage covers the landscape of Indian dental insurance in more detail. For specific coverage questions, checking your policy document or calling the insurer directly before the appointment is always advisable.
FAQ 3: What is the success rate of root canal treatment?
Root canal treatment has a well-established success rate of approximately 85 to 95 percent for primary treatment — meaning the treated tooth remains functional and symptom-free at five to ten years follow-up. Success rates depend on the initial condition of the tooth, the complexity of the root anatomy, the quality of the restoration placed after treatment, and the patient’s oral hygiene going forward. Teeth treated early — before the infection has spread significantly beyond the root tip — have higher success rates than those treated after a large abscess has formed.
FAQ 4: Does a root canal weaken the tooth permanently?
Root canal treatment does change the tooth’s structure — the pulp tissue that provided moisture to the tooth’s internal structure is removed, which makes the tooth somewhat more brittle than a vital tooth over time. This is precisely why a crown is recommended after root canal treatment for most back teeth: the crown prevents the tooth from fracturing under normal biting forces. A properly crowned tooth that has had root canal treatment can function for decades without issue. The brittleness of an uncrowned root canal tooth — not the root canal itself — is the primary risk factor for long-term failure.
FAQ 5: If I have a root canal now, can I still get an implant later if it fails?
Yes. If a root canal-treated tooth eventually fails — whether due to fracture, reinfection, or other causes — extraction and implant placement remain options at that point, provided adequate bone volume is present. Keeping the tooth with root canal treatment does not compromise future implant options, and in fact helps preserve the bone volume that makes implant placement straightforward. This is one of the reasons the clinical preference is always to attempt to save the tooth first: extraction eliminates options, while root canal treatment preserves them. Learn more about dental implants at Nova Dental Hospital, or visit our Google Business Profile to read what patients say about their experience.
🔑 Key Takeaways
- Root canal treatment and extraction are not equivalent alternatives — they have fundamentally different consequences for your bone, your adjacent teeth, and your long-term oral health.
- Extraction is rarely the end of the story. For most teeth, a gap needs to be managed, and the realistic cost of extraction plus replacement frequently exceeds the cost of saving the tooth.
- The clinical decision between root canal and extraction is made on specific factors: restorability, bone levels, root anatomy, and the patient’s broader oral health context. It is never a generic choice.
- The fear that root canal treatment is uniquely painful is not supported by the experience of patients treated under modern anaesthesia and technique. The tooth pain that precedes treatment is typically worse than the procedure itself.
- When extraction is the right answer — vertical fractures, severe bone loss, non-restorable teeth — it is the right answer regardless of the general preference for saving teeth. The goal is always the best outcome for the patient’s overall oral health.
Conclusion: Save the Tooth Where You Can — and Make the Decision With Full Information
The decision between root canal treatment and extraction is one of the most consequential choices a dental patient makes. It is also one of the most commonly made on incomplete information — with the extraction appearing deceptively simple and the root canal appearing deceptively complicated.
The clinical principle is straightforward: a natural tooth that can be saved should be saved. Not because root canal treatment is always the easier path in the short term, but because the long-term consequences of losing a tooth — bone loss, tooth movement, replacement cost, and functional change — are real, cumulative, and entirely predictable from the moment the tooth is extracted.
The cases where extraction is genuinely the correct clinical recommendation are specific and clear. Where those criteria are not met — where the tooth is restorable and the bone is adequate — the preference for saving the natural tooth is not sentiment. It is evidence-based dentistry. A consultation at Nova Dental Hospital will give you a complete clinical picture of your specific situation: the condition of the tooth, the bone levels, the realistic prognosis of each option, and an honest assessment of the costs involved. The decision is yours — but it should be made with accurate information.
Related posts


Write a Comment
Recent Posts




