
What Happens to Your Jawbone When You Lose a Tooth — and Why Timing Matters
What Happens to Your Jawbone When You Lose a Tooth — and Why Timing Matters
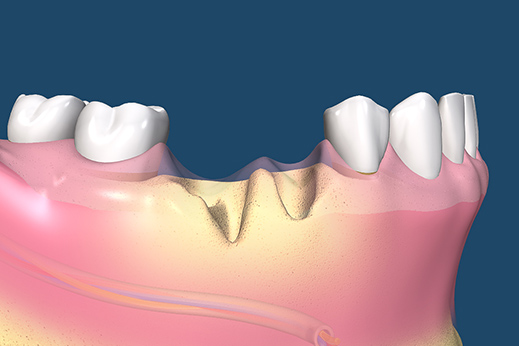
The gap left by a missing tooth is visible. The bone loss beneath it is not — but it is the consequence that shapes every future treatment option, and it begins within weeks of extraction.
The Consequence of Tooth Loss That Nobody Explains at the Time
When a tooth is extracted, the focus is — understandably — on the immediate situation: managing the procedure, controlling any infection, relieving the pain that prompted the extraction. What is almost never discussed at the time of the extraction is what happens next — not to the gap in the smile, but to the jawbone beneath it.
Bone loss following tooth extraction is not an occasional complication. It is a predictable, universal biological response. The jawbone that surrounded and supported the tooth root begins to resorb — to break down and diminish — from the moment the root is removed. This process starts within days, accelerates in the first three months, and continues at a slower rate for years. The longer a tooth is missing without replacement, the more bone is lost. And bone, once lost, cannot be fully recovered without grafting procedures that add complexity, cost, and time to any future treatment.
For patients considering what to do about a missing tooth — or for patients who have had a tooth missing for some time — understanding this process is the most clinically important thing they can know. It directly affects which treatment options are available, how complex those options will be, and whether an implant — the replacement option that most closely replicates a natural tooth — remains feasible. This guide explains the biology of bone resorption, the timeline of loss, the consequences for surrounding teeth and facial structure, what can prevent or slow the process, and why the timing of replacement matters as much as the choice of replacement.
🔑 Key Takeaways
- Jawbone resorption — the progressive loss of bone volume in the jaw after tooth extraction — is a universal biological response that begins within days of extraction and continues for years.
- In the first year after extraction, approximately 25 percent of bone width and 4 millimetres of bone height are lost on average. After three years, bone volume reduction of 40 to 60 percent has been documented.
- The root of a natural tooth transmits biting forces to the surrounding bone, stimulating bone cell activity and maintaining bone density. When the root is removed, that stimulation stops and the bone begins to resorb — a process called disuse atrophy.
- Dental implants are the only tooth replacement that replicates the mechanical stimulation of a natural root and thereby halts bone resorption. Bridges and dentures replace the visible crown but allow bone loss beneath the replacement to continue.
- Socket preservation — placing a bone graft into the extraction socket at the time of extraction — significantly reduces the rate of bone resorption and preserves options for future implant placement.
- The timing of replacement matters more than most patients realise. An implant placed within a few months of extraction is simpler, cheaper, and more predictable than one placed after years of bone loss that may have left insufficient bone for straightforward placement.
The Biology: Why Bone Disappears When a Tooth Is Lost
Bone as a Dynamic, Load-Responsive Tissue
Bone is not static. It is living tissue that continuously remodels in response to the mechanical forces it experiences — a process governed by two cell types: osteoblasts (bone-building cells) and osteoclasts (bone-resorbing cells). In healthy bone, these two cell populations are in balance, maintaining bone density and volume in proportion to the functional demands placed on the tissue.
This responsiveness to load is well established across the body. Astronauts who spend extended periods in zero gravity lose significant bone density because the skeletal system is no longer subjected to gravitational loading. Athletes who train with heavy resistance loads develop higher bone density in the loaded areas. The principle — bone maintains itself in proportion to the load it receives — is one of the most fundamental in musculoskeletal biology.
How the Tooth Root Stimulates the Bone
The root of a natural tooth is surrounded by the periodontal ligament — a thin layer of specialised connective tissue fibres that anchor the root to the surrounding alveolar bone. These fibres are not simply mechanical tethers; they are mechanosensory structures that transmit the compressive and tensile forces of chewing and biting directly to the bone cells in the socket wall.
Every time a force is applied to the tooth — chewing, biting, swallowing — the periodontal ligament fibres transmit that load to the alveolar bone. The bone cells respond to this stimulation by maintaining their remodelling activity. Osteoblasts lay down new bone matrix; osteoclasts remodel it; the net result is that the bone volume and density around the root is actively maintained by the functional demands of the tooth.
What Happens When the Root Is Removed
When a tooth is extracted, two things happen simultaneously. The root — the mechanical stimulator of the surrounding bone — is removed. And the periodontal ligament fibres that connected the root to the bone are disrupted and lost. The alveolar bone that surrounded the root suddenly has no functional load being transmitted to it and no periodontal ligament signalling its maintenance.
The osteoclast-osteoblast balance shifts. Without functional stimulation, osteoclast activity (resorption) dominates over osteoblast activity (formation). The bone begins to break down — first the thin bony walls of the socket, then the surrounding alveolar ridge. This is not pathological; it is the bone responding appropriately to the absence of functional demand. But from the patient’s perspective, the result is progressive, irreversible loss of the bone that would be needed to support a future implant.
The Timeline of Bone Loss — What Happens and When
The First Few Weeks — Socket Healing
In the days immediately after extraction, the socket fills with a blood clot that organises into granulation tissue — the first stage of wound healing. The thin bony walls of the socket (the bundle bone, which was intimately associated with the periodontal ligament) begin to resorb within the first week. This early resorption is part of normal socket healing and cannot be prevented, even with a graft placed at the time of extraction.
Months One to Three — The Period of Most Rapid Loss
The most dramatic bone loss occurs in the first three months after extraction. Clinical studies consistently document:
- Horizontal width loss of 29 to 63 percent of the original socket width in the first three months
- Vertical height loss of 11 to 22 percent of the original socket height in the same period
- Greatest resorption on the buccal (cheek-facing) surface — the thinner outer wall of the socket resorbs faster than the thicker palatal or lingual wall, producing a ridge that is not only narrower but also repositioned lingually (towards the tongue)
This is the period during which timely intervention — socket preservation grafting, early implant placement — makes the greatest clinical difference. By the end of the third month, a significant proportion of the bone that would be needed for a straightforward implant placement may already be lost.
Three Months to One Year — Continued Resorption
Resorption continues beyond the initial rapid phase, albeit at a slower rate. By the end of the first year after extraction, the average alveolar ridge has lost approximately 25 percent of its original width and 4 millimetres of height. These are averages — individual variation is significant, and patients who had thin buccal bone, gum disease, or infection at the time of extraction may lose substantially more.
Years One to Three and Beyond — Long-Term Atrophy
Long-term studies following patients for three years after extraction document total bone volume reductions of 40 to 60 percent compared to the pre-extraction state. The ridge that remains is not only narrower and shorter but may have changed in shape — the concave morphology of advanced resorption creates a topography that complicates implant placement and may require additional grafting procedures to restore the site to a shape suitable for implant surgery.
For patients with multiple missing teeth, the cumulative bone loss across multiple sites, combined with the functional overloading of the remaining teeth, can produce significant changes to the facial structure — the lower face appears shorter, the cheeks lose support, and the jaw appears to protrude as the upper and lower ridges resorb differentially.
| Time After Extraction | Bone Width Loss | Bone Height Loss | Clinical Implication |
| First 3 months | 29–63% of original width | 11–22% of original height | Most critical window for intervention — socket preservation or early implant placement |
| 3–12 months | Continues at slower rate | 4mm average height loss at 1 year | Implant still feasible in most cases; may need minor grafting |
| 1–3 years | Up to 40% total width reduction | Significant vertical loss | Implant often requires bone grafting; more complex procedure |
| 3+ years | 40–60% total volume loss | Ridge morphology significantly altered | Major grafting often required; some cases require sinus lift or ridge augmentation |
| Long-term (denture wearers) | Severe; ongoing under denture pressure | Progressive with denture use | Remaining ridge may be insufficient for implant without extensive reconstruction |
The Downstream Consequences — What Else Bone Loss Affects
Adjacent Tooth Stability
The alveolar bone that resorbs after tooth loss is not confined to the extraction site. The bone loss gradually affects the support around the roots of adjacent teeth, particularly if the gap is left unmanaged for years. Adjacent teeth that lose supporting bone become progressively more mobile and more susceptible to the forces of chewing — particularly if they are also bearing the additional load that the missing tooth used to share.
Tooth Drifting and Bite Changes
As discussed in our blog on space maintainers for children, the teeth adjacent to a gap begin to drift into the space. This is not limited to children — adult teeth drift too, though more slowly. The tooth behind the gap moves mesially (forwards); the tooth in front of the gap tips distally (backwards); the opposing tooth supra-erupts (moves downward or upward into the gap). These movements alter the bite, create new areas of uneven force distribution, and can produce TMJ symptoms, accelerated wear on the remaining teeth, and further bone loss at the drifted sites.
Facial Structure Changes
The alveolar bone — the tooth-bearing portion of the jaw — contributes significantly to facial height and contour. When multiple teeth are lost and the alveolar bone resorbs, the lower face loses vertical height. The lips lose support and begin to fold inward. The chin appears to move forward relative to the nose. These changes are gradual and typically go unnoticed year to year — patients see them only when comparing photographs taken a decade apart and are often surprised at how significantly their facial appearance has changed in the absence of their natural teeth.
For patients who have been wearing conventional complete dentures for many years, this progressive bone resorption beneath the denture — accelerated by the pressure of the denture base on the ridge — can make denture retention increasingly difficult and the facial changes increasingly pronounced. This is one of the most clinically compelling arguments for implant-retained dentures over conventional ones — the implants halt the resorption process beneath the prosthetic.
Implant Feasibility
Perhaps the most practically significant consequence of bone loss for patients considering tooth replacement is its effect on implant feasibility. A dental implant requires a minimum bone volume — typically at least 10 mm of height and 6 mm of width — to be safely placed and to integrate successfully. When bone has resorbed significantly below these thresholds, implant placement requires bone grafting before or concurrent with surgery — adding complexity, cost, healing time, and a degree of clinical unpredictability to what would otherwise be a straightforward procedure.
The patient who presents for an implant assessment with a tooth that was extracted six months ago typically has sufficient bone for straightforward placement. The patient who presents with a tooth that was extracted five years ago, with no graft at the time of extraction, frequently requires a staged bone grafting procedure before implant placement is possible — adding three to six months and significant additional cost to the treatment plan.
What Can Prevent or Slow Bone Loss
Socket Preservation Grafting at the Time of Extraction
The most effective intervention for preventing post-extraction bone loss is socket preservation grafting — placing a bone graft material into the extraction socket at the time of the extraction, before the wound is closed. The graft material — which may be synthetic, bovine-derived, or processed human bone — acts as a scaffold that fills the socket space and slows the resorption of the socket walls during healing.
Studies comparing grafted and ungrafted sockets consistently show that socket preservation reduces horizontal bone width loss from an average of 3.8 mm to approximately 1.5 mm, and vertical height loss from 1.7 mm to 0.5 mm. This is not a complete prevention of bone loss — the bundle bone resorbs regardless — but it preserves the bulk of the alveolar ridge in a form that is much more amenable to implant placement without additional grafting.
Socket preservation is a relatively simple addition to an extraction procedure and adds minimal recovery time. It is most valuable when an implant is planned for the future but is not being placed immediately — giving the site time to heal in a preserved form before implant placement.
Immediate or Early Implant Placement
An alternative to grafting alone is the placement of the implant fixture into the extraction socket immediately after — or within a few weeks of — the extraction. Immediate implant placement preserves bone by reintroducing functional stimulation to the socket before significant resorption occurs. It also reduces the total treatment time — the patient goes from extraction to implant in a single surgical procedure rather than two separate procedures with a healing period between them.
Immediate implant placement is not appropriate for every case — it requires specific bone volume, bone quality, and socket anatomy to be predictable — and a CBCT 3D assessment is essential to determine whether the site is suitable. Where appropriate, it is one of the most clinically efficient approaches to tooth replacement, preserving bone while minimising surgical appointments and total treatment time.
Implant Placement (Even After a Gap)
For patients who have already had a tooth missing for some time without grafting or replacement, implant placement — even if bone grafting is now required — halts the resorption process from the point of placement. An integrated implant transmits functional load to the bone exactly as a natural root does, stopping the disuse atrophy and maintaining the bone volume around the implant for decades. This is one of the most important long-term arguments for implant replacement over bridges or dentures — the bone preservation effect continues for the life of the implant.
What Bridges and Dentures Do to Bone
A dental bridge replaces the visible crown of the missing tooth by anchoring crowns on the adjacent teeth and spanning the gap with a false tooth (pontic). The bone beneath the pontic receives no stimulation — the bite forces are transmitted through the abutment crowns to the adjacent roots, not to the bone beneath the gap. Bone loss beneath a dental bridge continues unimpeded, and over years, a depression develops in the ridge beneath the pontic that becomes increasingly visible as the gum tissue drops away from the pontic margin.
A conventional removable denture transmits compressive forces to the ridge surface through the denture base — forces that accelerate, rather than maintain, bone resorption. Patients who have worn a conventional complete denture for twenty years may have lost the majority of their alveolar bone, leaving a flat or concave ridge that barely supports the denture and makes any future implant placement extremely complex.
💡 The Replacement Options and Their Effect on Bone — A Summary
- No replacement (gap left open): Bone loss continues at the maximum natural rate. Adjacent teeth drift. All future options become more complex and expensive over time.
- Removable partial denture: No bone preservation effect beneath the gap. Denture pressure may accelerate surface bone loss. Maintains aesthetics and some function but does not address the underlying biological process.
- Dental bridge: No bone preservation beneath the pontic. Bone loss continues under the gap. Requires preparation of healthy adjacent teeth. Long-term bone depression beneath pontic typically becomes visible.
- Dental implant: The only replacement that halts bone resorption by reintroducing functional stimulation to the alveolar bone. Preserves bone for the life of the implant. Requires sufficient bone at placement — or grafting if bone has already been lost.
- Socket preservation graft (at extraction): Significantly reduces bone loss in the critical first months. Not a tooth replacement itself — it preserves the site for future implant placement at the optimal time.
The Role of CBCT Imaging in Assessing Bone Loss
For patients who are missing a tooth and considering implant replacement — whether recently extracted or missing for years — the most important first step is an accurate three-dimensional assessment of the bone that remains. A conventional two-dimensional OPG X-ray shows bone height but does not reveal bone width or the three-dimensional morphology of the ridge.
A CBCT 3D scan at Nova Dental Hospital provides the complete picture — height, width, density, and shape of the available bone in the implant site, the distance to the inferior dental nerve in the lower jaw, the height of bone below the sinus in the upper jaw, and the presence of any anatomical factors that affect surgical planning. This imaging allows the implant clinician to determine:
- Whether sufficient bone is present for straightforward implant placement
- Whether bone grafting is needed before or at the time of implant placement
- What type of graft, what dimensions, and what approach would best reconstruct the site
- The optimal implant dimensions, angulation, and position for the available bone
- Whether a surgical guide can be fabricated for precise, safe implant placement
Having this imaging in-house — rather than as an external referral — means the clinician planning the treatment has immediate, integrated access to the three-dimensional data at the consultation appointment, allowing a treatment plan to be developed and discussed in the same visit.
Frequently Asked Questions
FAQ 1: How long can I wait before getting an implant after a tooth extraction?
There is no absolute deadline — implants can be placed years after extraction, including in patients with significant bone loss who need grafting. However, the longer you wait, the more bone is lost and the more complex the implant procedure becomes. Within the first three months, bone loss is most rapid. Acting within six months of extraction — either with socket preservation grafting or early implant placement — preserves the most bone and gives the simplest, most predictable treatment pathway. Waiting more than a year without any grafting means bone augmentation is likely to be needed before implant placement. A CBCT assessment at Nova Dental Hospital will give you an accurate picture of what bone remains and what options are available at any point in time.
FAQ 2: I had a tooth extracted years ago and never replaced it. Is it too late for an implant?
In most cases, no — but the treatment may be more complex than it would have been earlier. A CBCT scan will determine how much bone remains and whether grafting is required before implant placement. Many patients who have had missing teeth for five or ten years can still receive implants, either with simultaneous bone grafting or with a staged grafting procedure before implant placement. The assessment is the only way to know what is feasible in your specific case. For complex cases involving multiple missing teeth and significant bone loss, full mouth rehabilitation planning gives the most comprehensive picture of what is achievable.
FAQ 3: Does a dental bridge prevent bone loss under the gap?
No. A conventional dental bridge replaces the visible crown of the missing tooth but does not provide the mechanical stimulation that prevents bone resorption beneath the gap. The bone under the pontic (the false tooth spanning the gap) continues to resorb, and over years a depression develops in the ridge beneath the pontic as the gum tissue drops away from the unsupported surface. For patients who choose a bridge over an implant for any reason, this bone loss is an accepted trade-off rather than a complication — but it is important to understand that the bridge does not halt the underlying biological process the way an implant does. The crown and bridge page has further information on bridge treatment at Nova Dental Hospital.
FAQ 4: What is socket preservation and should I ask for it when having a tooth extracted?
Socket preservation is the placement of a bone graft material into the extraction socket at the time of extraction, before the wound is closed. It significantly reduces the bone width and height loss that would otherwise occur in the first months after extraction, preserving a more favourable site for future implant placement. Whether it is appropriate depends on whether you are planning an implant in the future. If you intend to replace the tooth with an implant, socket preservation at extraction is strongly worth considering — it is a relatively simple addition to the extraction procedure and can save the need for a more complex grafting procedure later. If you are not planning an implant, the additional intervention may not be warranted. Discuss this with the dentist at the extraction appointment — the decision is most useful when made before extraction, not after.
FAQ 5: How do I know if I have enough bone for a dental implant in Gandhinagar?
The only accurate way to assess this is with a CBCT 3D scan, which maps the height, width, and density of the bone in three dimensions. A two-dimensional X-ray can estimate height but does not reveal width or morphology — two patients with the same bone height on an OPG may have very different bone widths that dramatically change the treatment plan. Nova Dental Hospital has an in-house CBCT facility that allows bone assessment and virtual implant planning at the same consultation appointment. Book an implant assessment and the team will give you a precise, specific answer for your case. You are welcome to read about implant patient experiences on our Google Business Profile.
🔑 Key Takeaways
- Bone resorption after tooth extraction is universal, predictable, and progressive — beginning within days and continuing for years. It is not a complication; it is normal biology. But its consequences for future treatment options are significant.
- The first three months are the period of most rapid bone loss — up to 63 percent of ridge width can be lost in this window. This is also the period when timely intervention makes the greatest clinical difference.
- Socket preservation grafting at the time of extraction significantly reduces bone loss and preserves the site for future implant placement — at minimal additional complexity compared to the extraction itself.
- Dental implants are the only replacement option that halts bone resorption by reintroducing functional stimulation to the alveolar bone. Bridges and dentures leave bone loss beneath the replacement unchecked.
- The longer a tooth is left missing without grafting or replacement, the more complex, costly, and time-consuming the eventual implant treatment becomes. Timing matters more than most patients realise at the point of extraction.
- A CBCT 3D scan is the starting point for any implant assessment — it gives the precise three-dimensional bone picture that determines what is feasible and what is needed.
Conclusion: The Decision Made at Extraction Shapes Everything That Follows
When a tooth is extracted, the focus is on the problem being solved in that moment. The conversation about what comes next — about the bone loss that is now beginning, about socket preservation, about the window for implant placement, about what happens if the gap is left — is the conversation that should happen at the same appointment, and too often does not.
Understanding bone resorption gives patients the information they need to make better decisions about replacement timing. Not because every patient needs an immediate implant — the right timing depends on the clinical situation, the health of the site, and the patient’s own priorities — but because understanding the biology means the decision is made consciously rather than by default. A patient who chooses to wait knows what they are trading off. A patient who chooses socket preservation knows why it is worth the additional investment at the extraction stage.
If you have recently had a tooth extracted and want to understand your options — or if you have had a tooth missing for some time and are now considering replacement — a consultation at Nova Dental Hospital gives you the complete clinical picture. The in-house CBCT scan tells you exactly how much bone remains. The team will outline the most appropriate pathway from that starting point — whether that is straightforward implant placement, bone grafting before implant placement, or another approach. Book an appointment with one of the best dental clinics in Gandhinagar and make an informed decision.
Related posts


Write a Comment
Recent Posts




